

Summary
Some clinically important species of the Borrelia family include Borrelia burgdorferi and Borrelia recurrentis.
Some clinically important species of the Borrelia family include Borrelia burgdorferi and Borrelia recurrentis.
Virulence and microbiologic features:
- Borrelia is a corkscrew-shaped spirochete [1]
- It exhibits poor gram staining [2]. However, Giemsa and Wright staining can help visualize the organism [1].
- It is microaerophilic [3] and motile [4].
- White-footed mice and white-tailed deer are reservoirs for Borrelia burgdorferi [1].
- Wild rodents in the western U.S. are reservoirs for relapsing fever causing Borrelia species [6].
- Borrelia species responsible for relapsing fever have devised mechanisms to evade opsonization and phagocytosis by the immune system. One such mechanism is the antigenic variation of Vmp lipoproteins in the outer membrane of the Borrelia [5,6]
Transmission:
- Transmission of Borrelia burgdorferi responsible for Lyme disease is through Ixodes pacificus tick on the West Coast and through Ixodes scapularis in the East and Midwest [6].
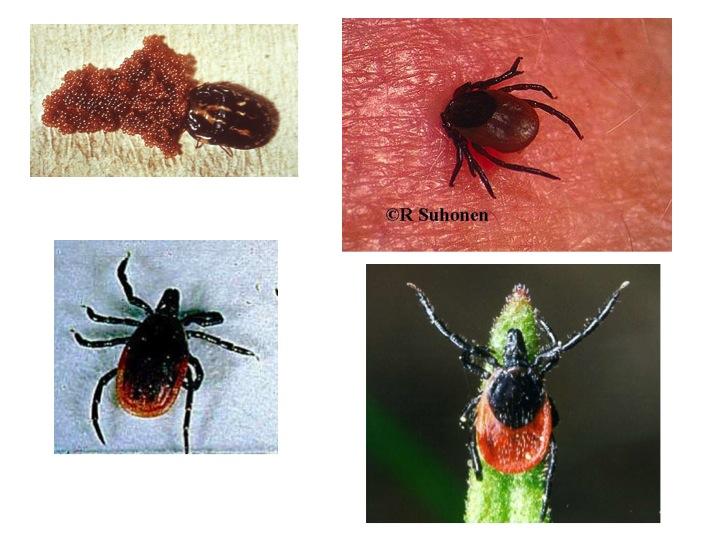
Ixodes (hard ticks) (14854411069) by Michael Wunderli is licensed under CC BY 2.0.
- For Borrelia species responsible for causing relapsing fever, Pediculus humanus (body louse) is a vector for Borrelia recurrentis, and Ornithodoros tick is a vector for other species [5].

Ornithodoros (soft ticks) by Michael Wunderli is licensed under CC BY 2.0.
Diseases and complications:
Lyme disease:
Borrelia burgdorferi causes lyme disease. The patient can have the following three stages of the disease [1]:
- Early localized stage: A few days after the tick bite, the patient develops erythema migrans at the site of the tick bite. It is a circular lesion with a red border and central clearing and gradually increases in size [1].

OSC Microbio 12 02 LymeRash by CNX OpenStax is licensed under CC BY 4.0.
Enlargement of regional lymph nodes, fever, and muscle aches can also occur. This stage can last up to a month [7].
- Early disseminated stage: Hematogenous spread of Borrelia burgdorferi occurs to other body organs such as the nervous system, joints, and heart. Clinically, this can manifest as multiple erythema chronicum migrans and neurological symptoms such as aseptic meningitis or bell’s palsy. Cardiac involvement can also lead to transient heart block. Additionally, musculoskeletal manifestations like migratory arthralgias and myalgias may occur due to joint and muscle involvement [1,8].
- Late stage: This stage can develop in some untreated patients, and possible clinical manifestations of this stage include encephalopathy and chronic arthritis of large joints (such as the knee) [8].
Relapsing fever:
After the incubation period, the patient develops a recurrent fever, chills, muscle aches, and headaches. These symptoms typically subside within a week, coinciding with the clearance of bacteria from the bloodstream. However, they may reoccur after a one-week interval [9].
Diagnostic testing:
- Dark field microscopy and Giemsa- or Wright-staining are helpful for the diagnosis of relapsing fever during febrile episodes. However, microscopy is not preferred for Lyme disease [9,10].
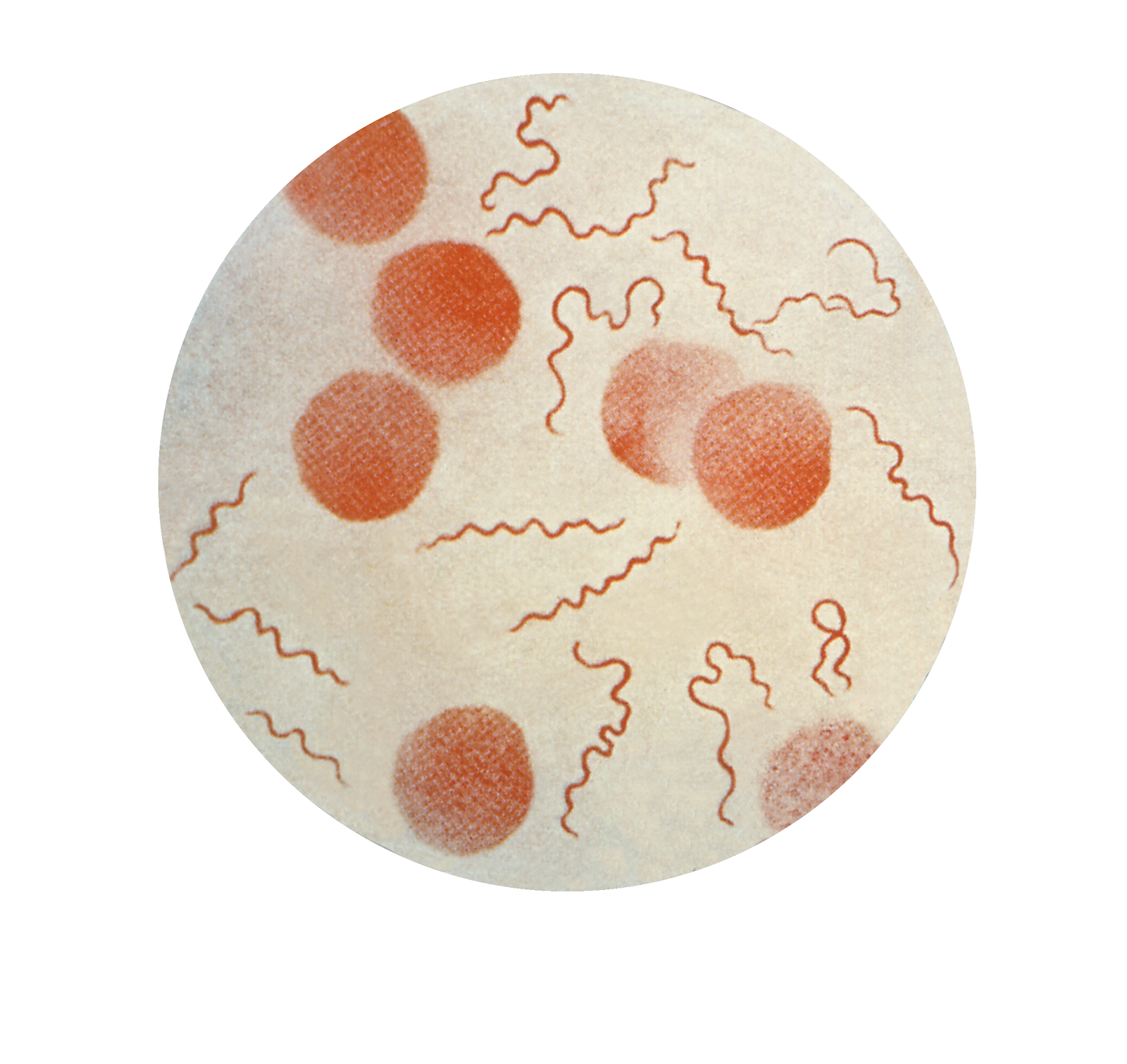
File:Borrelia recurrentis CDC.png by CDC is marked with CC0 1.0.
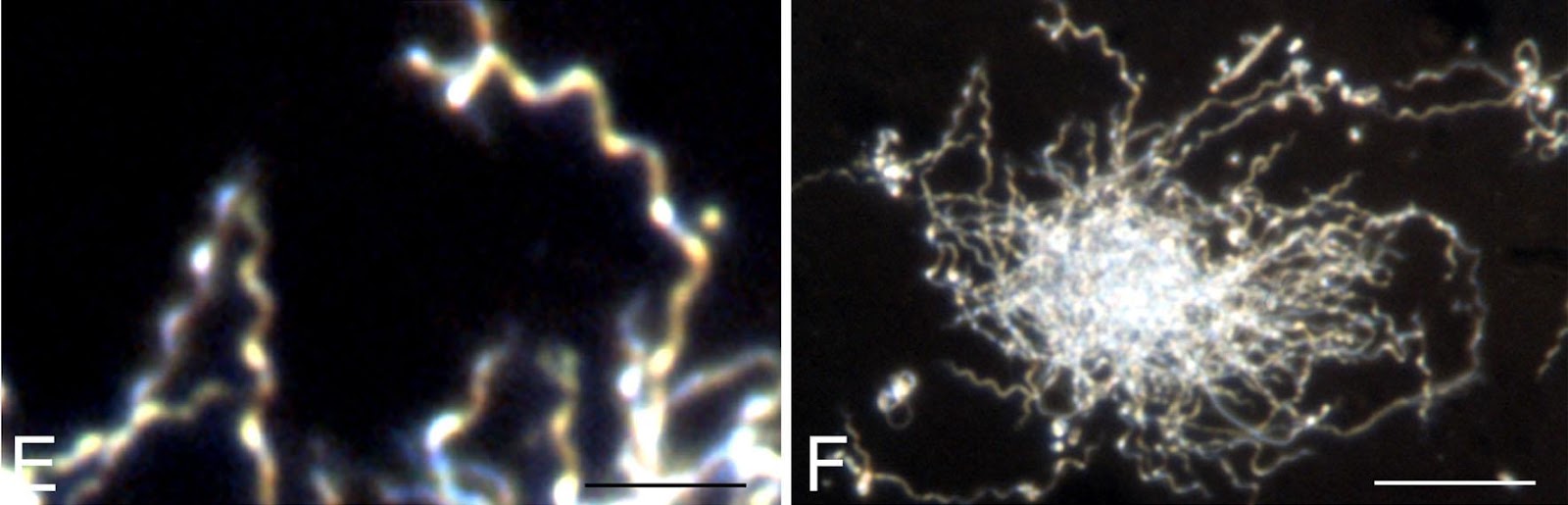
File:Borrelia dark field.jpg by Judith Miklossy, Sandor Kasas, Anne D Zurn, Sherman McCall, Sheng Yu and Patrick L McGeer is licensed under CC BY 2.0.
- Serological testing such as immunofluorescence assay and enzyme immunoassays can detect elevated antibody levels. Serological tests are preferred for Lyme disease but are not helpful in relapsing fever [9].
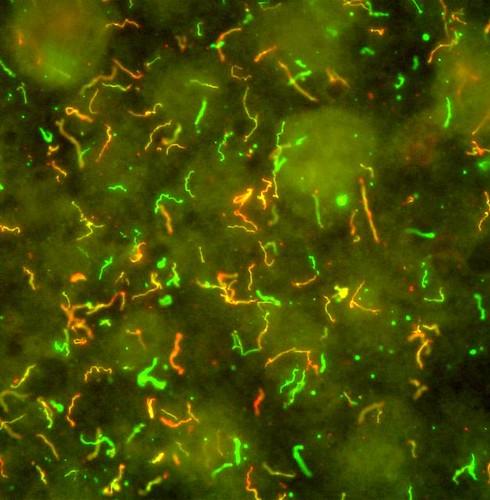
Lyme Disease Bacteria, Borrelia burgdorferi by NIAID is licensed under CC BY 2.0.
References:
- CMMRS edition 6, 2016-17 (page no: 134)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 327)
- CMMRS edition 6, 2016-17 (page no: 138)
- Jawetz, Melnick, & Adelberg’s Medical Microbiology Twenty-Seventh Edition (page no: 327)
- CMMRS edition 6, 2016-17 (page no: 136)
- CMMRS edition 6, 2016-17 (page no: 140)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 329)
- CMMRS edition 6, 2016-17 (page no: 135)
- Medical Microbiology by Patrick R. Murray Ph.D., Ken Rosenthal Ph.D., Michael A. Pfaller MD, 8th edition (page no: 330)
- CMMRS edition 6, 2016-17 (page no: 141)